
1-RM Testing in Rehabilitation
The role of Max Strength Testing
Understanding the maximum capacity of a muscle group is critically important for dosing resistance exercise. One repetition maximum (1-RM) is essentially the benchmark for prescribing load — in every setting — from rehabilitation to sport performance.
Programming Guide
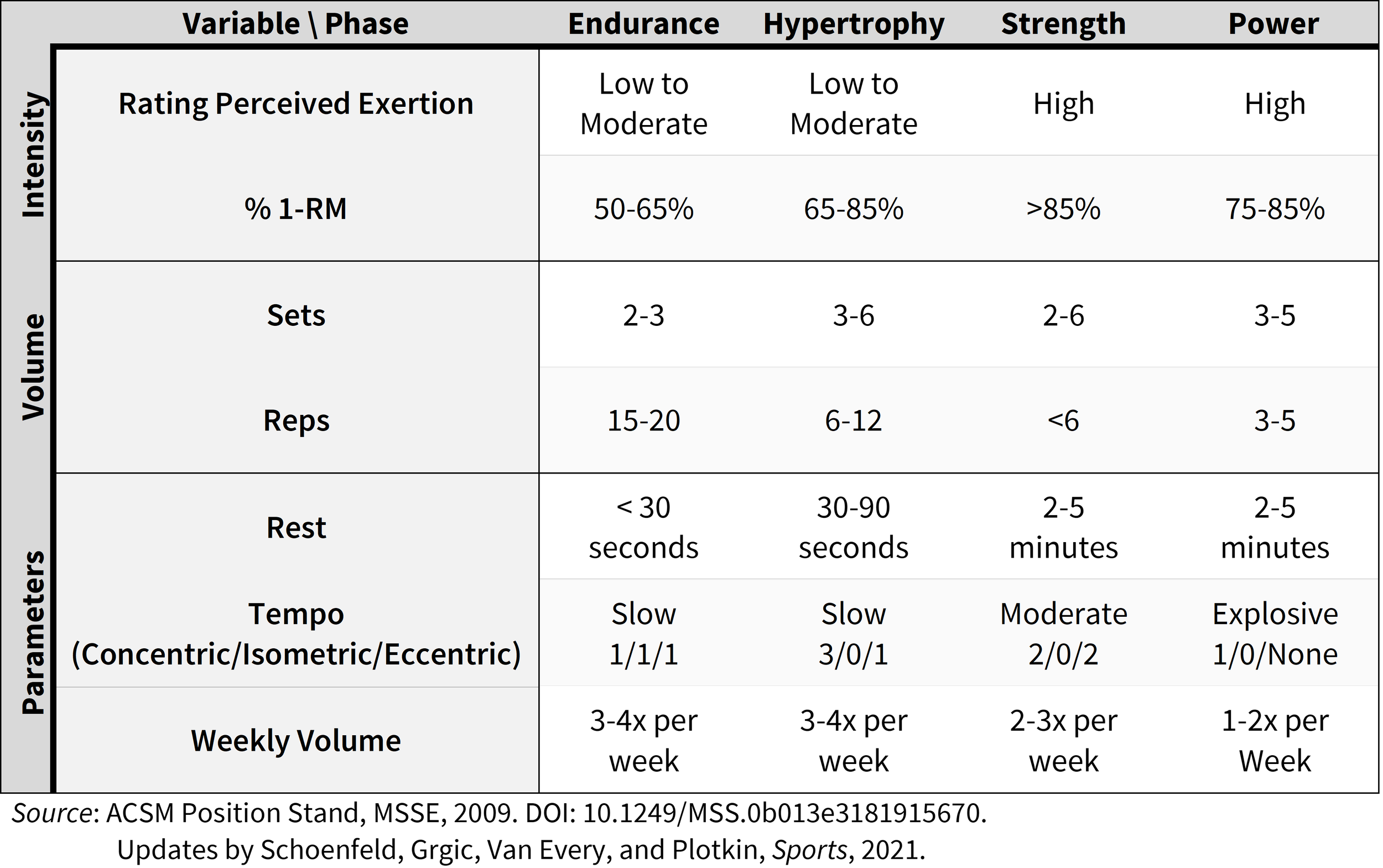
Programming, from rehabilitation to strength and conditioning, depends upon progressive overload principles to stimulate muscle adaptation. The American College of Sports Medicine offers their gold standard position stand for training based on years of foundational research (Table).
1-RM is the benchmark
As you can see, the 1-RM is the benchmark for determining load/intensity for all resistance training goals — i.e., endurance, hypertrophy, strength, or power. Without it, coaches, therapists, and individuals rely on estimation of weight selection during their workouts. At Live4 Physical Therapy and Wellness, we believe exercise is medicine. Would you take a prescription that whose dose was ‘estimated’ to work for you? Our clients deserve better than estimation.
In contrast, traditional 1-RM testing is not suited for everyone — in fact, maximal effort lifts can rarely be used safety in rehabilitation settings due to poor load tolerance secondary to injury. For that reason, we recommend applying submaximal 1-RM testing to determine 1-RM load and customize programming according. Submaximal 1-RM testing is repeatedly shown to be just as good as traditional 1-RM testing (Grgic et al., Sports Medicine - Open, 2020).
Submaximal 1-RM Testing
To complete submaximal 1-RM testing, a person performs a given exercise to failure. The load should be selected so that failure is achieved in 10 reps or less (can be more, but it opens up the chance for more error in the prediction). The weight lifted is then multiplied by a constant to predict the individual’s 1-RM.
Sound too easy? It is.

Chart depicting submaximal conversion to 1 repetition maximum for strength and conditioning and rehabilitation.
Example procedures submaximal 1-RM Testing:
Start at perceived 8-RM or 10-RM load
Perform reps to failure or fatigue
If >10 reps are performed, take 2 minutes rest and increase the weight by 5-10%.
If 10 or fewer reps are performed, you did it!
Convert the weight lifted to Predicted 1-RM using the adjustment equation:
Essentially, multiply weight lifted in submaximal testing by the conversion factor.
If 10 repetitions, then Predicted 1RM = 10RM weight * 1.33
The conversion factor ranges from 1.05 (for 2 reps completed) to 1.33 (for 10 reps completed).
Examples: [ (Weight lifted) x Rep # Conversion Constant = Predicted 1-RM ]
3 reps lifted with 20 kgs during a knee extension: (20 kg) * 1.08 = 21.6 kg
5 reps lifted with 20 pounds during a biceps curl: (20 lbs) * 1.14 = 22.8 lbs
7 reps lifted with 35 pounds during an overhead press: (35 lbs) * 1.21 = 42.4 lbs
Then plug the 1-RM into your programming: [ 1-RM * % 1-RM for Exercise Goal = Ideal Load ]
Goal of Quadriceps Strength: 21.6 kg * 0.90 = 19.4 kg
Goal of Biceps Endurance: 22.8 lbs * 0.65 = 14.82 lbs
Goal of Overhead Press Power: 42.3 lbs * 0.80 = 33.8 lbs
Small change. Big results.
Simple practices like taking the time to assess 1-RM every few weeks can have a huge impact on progress in rehabilitation. Underloading is far too common in rehabilitation and amounts to a waste of time and slow progress. Overloading is dangerous, but easy to avoid with 1-RM screening.
Effective clinicians use the progressive overload framework to guide programming and meet recommendations for progressive strengthening. Submaximal 1-RM testing is a huge part of that!