
Cryotherapy User Guide
Disclosure: Some links in this post are affiliate links, which means we may earn a small commission at no additional cost to you. We only recommend products we personally use or recommend to our clients.
Using Cryotherapy for Focal Joint Cooling.
Nerve function is slowed at low temperatures. This makes icing a swollen and painful joint THE BEST way to address muscle inhibition. This has been shown in randomized controlled trials for patients with ACL reconstruction, as well as knee osteoarthritis. The bottom line: Use cryotherapy BEFORE exercise to improve efficacy of quadriceps strengthening work. Doing so has resulted in 38% increase in strength in just 2 weeks (Hart et al, JAT 2014).
How does cryotherapy work?
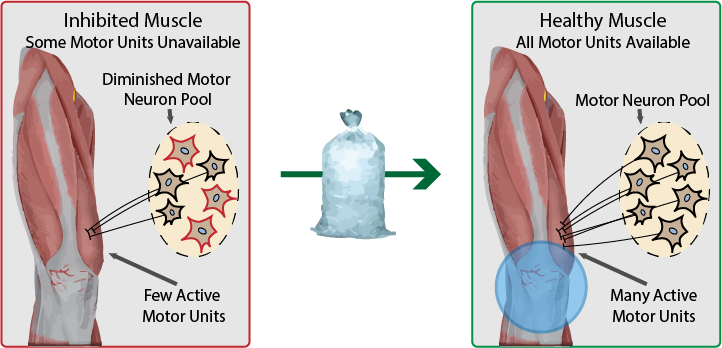
Remember this: as long as the sensory signal from the joint is disrupted, spinal reflexive inhibition is present. Inhibition is caused by pain and swelling signals flooding the spinal cord (think: tripped circuit breaker). Icing slows down nerve conduction, reducing impact of inhibition from the joint, and xing the circuit breaker. This means neural access to the muscle is restored (but only for as long as the tissue is cold).
Seems crazy. Does it really work?
Back in 2014, Hart et al proved it works in patients after ACLR. In a randomized controlled trial, they assigned patients to 3 groups: 1) cryotherapy only, 2) exercise only, and 3) cryotherapy + exercise and trained for 2 weeks.
What happened? Groups 1 and 2 made similiar improvements in quadriceps strength (+14%). Group 3 made HUGE improvements over the same time (+38%) - See for yourself below (left plot).
They also tested quadriceps volitional activation (e.g., ability to access full muscle capacity) and found improvements weren’t di erent than exercise alone. So what it all mean? Cryotherapy doesn’t fix activation failure overtime (e.g., when tissue is warm, inhibition persists), but it allows effective strengthening by creating a therapeutic treatment window where our patients can access greater % of their motor units.

When should I use cryotherapy?
It is critically important to apply cryotherapy directly to the knee-joint BEFORE exercise. 20 minutes should be enough to numb the tissue and reduce sensory nerve conduction. If you are nervous about exercising with a numb knee, keep the exercises simple (e.g., open chain knee extension, leg press, etc.) and save the more complex neuromuscular control exercises for later in the session.
How long does cryotherapy last?
Only until the tissue re-warms. Cryotherapy creates a “Therapeutic Window” of about 45 minutes.
Barriers and Tips for Effective Cryotherapy Use
Time - Don't have time in session to spend 20 minutes icing? Try asking your patients to arrive early, or have them ice in the car on the way to each treatment. Plus, emphasis that patients do this at home!
No Ice Machine - Don't have access to ice? Products like Freeze Sleeves can be kept in freezers. If no freezer is available, emphasize patients use cryotherapy at home prior to their home exercise program. In clinic, use TENS (another disinhibitory intervention with similiar effects).
Cold Intolerance/Allergy - Is your patient allergic or intolerant to ice? You'll have to select another disinhibitory intervention (e.g., TENS).
Patient isn't Buying-In - Is your patient skeptical or not interested in cryotherapy? The effects should be fairly visable. Try filming a quadriceps contraction at baseline (pre) and then again after ice (post). This pre/post visual comparision of contraction quality should be convincing enough!
It's Time to Focus on Other Goals - If you need to use in-clinic time working towards other goals, a patient can still use cryotherapy at home while focusing on quadriceps strength. Hopefully, if you've been using cryotherapy from the start - quadriceps strength won't be much of a focus in the long-term!
A Thought on Compounding Effects Over Time

*Transient increases in muscle activation (~45 minutes) means more motor unit recruitment + higher mechanical and metabolic stress. Strength exercise are more effective. In 2 weeks of training, this translated into a 38% increase in quadriceps MVIC. If continued throughout the first 12 weeks of rehabilitation, what would that look like? What if we combined these effects with the use of Neuromuscular Electrical Stimulation (NMES) and Blood Flow Restriction (BFR)?
Download this post as an infographic.
Want Expert Guidance on Your Specific Situation?
Cryotherapy, NMES, blood flow restriction — these are all effective tools for addressing muscle inhibition, but the right combination depends on your specific situation. If you are looking for personalized guidance from someone who specializes in muscle inhibition and weakness, our Persistent Weakness Consultation can help you understand what's driving your symptoms and chart a clear path forward, no matter where you live.